Giving patients Bluetooth blood pressure cuffs improves overall health outcomes, but technology alone cannot erase deep-seated racial disparities in clinical care.
Can smart devices fix systemic healthcare inequalities? Many digital health advocates argue that remote monitoring levels the playing field by bringing care directly into patients’ homes. But a new study reveals a sobering truth. Even when everyone gets the same high-tech tools, existing racial gaps persist.
This complicates the naive belief that digital tools are a cure-all for equity. It confirms that software and hardware merely sit on top of fractured social foundations. If Black patients still lag behind White patients in the same program, the bottleneck is not the technology. It is how the healthcare system interacts with different communities.
The equity illusion
Researchers analyzed a retrospective cohort of 503 patients (out of 550 enrolled) at a single urban academic primary care clinic between January 2022 and December 2024. The cohort was majority-minority, with a mean age of 58.3 years. African American patients made up 63.6% of the group, and 52.9% were male. Patients transmitted daily readings via Bluetooth, and clinicians adjusted medications monthly based on 2017 ACC/AHA guidelines.
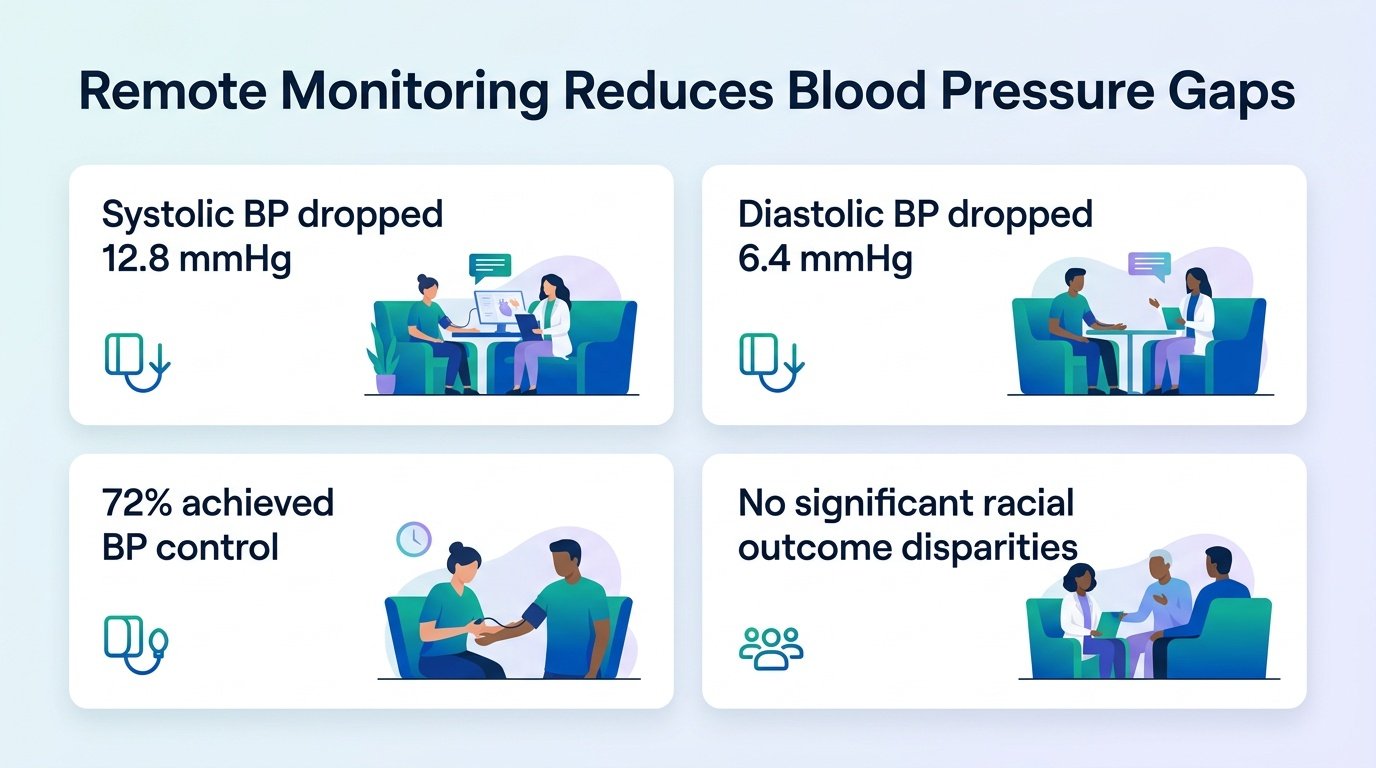
The program achieved a massive overall victory, but the underlying disparities remained stark. While overall control rates climbed, the gap between racial groups did not close.
- Overall blood pressure control rose from 10.1% at baseline to 37.1% at 9 months.
- Each month of enrollment cut the odds of uncontrolled blood pressure (adjusted odds ratio [aOR] 0.82).
- White patients had much lower odds of uncontrolled blood pressure than African American patients (aOR 0.57 for moderate control; aOR 0.40 for strict control).
- Male sex (aOR 1.46) and congestive heart failure (aOR 2.09 for strict control; aOR 2.05 for moderate control) predicted higher odds of remaining uncontrolled.
Why tech falls short
This pattern is not unique to this clinic. Similar implementation challenges have surfaced globally, as seen in London’s BP@home initiative, where primary care barriers often limit the reach of digital tools. To truly close these gaps, researchers are now designing trials specifically focused on safety-net systems, such as the REACH-SNS study.
We must view these findings with caution. The study was retrospective and lacked a concurrent usual-care control group, making it hard to prove direct causality. Because it took place at a single urban academic clinic, the results might not apply to rural or resource-poor settings.
However, the takeaway is clear. Giving a patient a Bluetooth cuff is only the first step. If health systems do not address the social factors that make it harder for minority patients to manage their health, digital medicine will only widen the divide.
Read the full study in medRxiv.